


 Case Report
Case Report - Patient Case Utilized as a Teaching Point During Community Pharmacy Experiential Rotation: Bleeding Risk and Drug Interactions of Warfarin
Sun Young Kim1* and Jun Woo Lee2
1Gomdallae Pharmacy, Gangseo-gu gomdallae-ro 226, Seoul, Republic of Korea, 07784
2Seoul National University, College of Pharmacy, Gwanak-gu, Gwanak-ro 1, Seoul, Republic of Korea, 08826- 약국 실무실습 교육 활용 환자 사례: 와파린의 출혈 위험성과 약물 상호작용
김선영1*, 이준우2
1곰달래약국, 서울 강서구 곰달래로 226, 07784
2서울대학교 약학대학, 서울시 관악구 관악로 1, 08826This article is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This case report summarizes the patient case of a long-term warfarin user experiencing bleeding hemorrhoids and bleeding risk and drug interactions of warfarin, which was used as a teaching point during experiential rotation at a community pharmacy. The patient was regularly taking warfarin 0.5~5 mg per day for dilated cardiomyopathy since 2010. In 2019, at age 74, he was diagnosed with bleeding hemorrhoids and had to stop taking warfarin. While low risk of drug-drug interactions was found within the prescribed cardiomyopathy drug regimen, cross-prescription reviews confirmed a high risk of drug-drug interactions. The combination of loop diuretics and NSAIDS may cause nephrotoxicity (major), and the combination of anticoagulants and NSAIDS may increase the risk of bleeding (major). The patient was at high-risk for bleeding based on the HAS-BLED score ≥ 3.0 (old age, unstable INR, bleeding, drugs) and NSAID-induced bleeding risk factors ≥ 2 (old age, high-dose NSAIDS, combined use of anticoagulants). In order to minimize drug-drug interactions and optimize safety, following interventions are recommended: 1) modification of warfarin to a novel oral anticoagulant (NOAC) to reduce bleeding risk, 2) modification of NSAID to an agent with low risk of gastrointestinal bleeding or concurrent use of a gastrointestinal protective agent, 3) patient education on warfarin-induced bleeding risk and lifestyle habits to prevent bleeding. This case report is meaningful in confirming the importance of patient medication management in pharmacy practice by examining the bleeding risk and drug interactions of warfarin through 10-years follow-up of the drug history of patient with cardiomyopathy.
Keywords: Community pharmacy, Pharmacy practice, Drug interaction, Warfarin, Warfarin-induced bleeding, Medication management
본 증례보고에서는 2019년 지역약국 필수 실무실습 중 발생한 warfarin 장기 복용중인 환자의 항문과다출혈 사례를 통해서 warfarin의 출혈 위험성과 약물상호작용을 조사하고 약사의 중재에 대해 교육시킨 사례를 소개한다. 본 실습약국의 형태는 인접한 병원이 없고 단골환자들이 다양한 병원의 처방전을 가지고 방문하는 지역약국이며, 장기간에 걸친 환자약력과 처방간 중복을 확인할 수 있는 장점이 있어서 만성질환자 또는 다제약물을 복용하는 환자사례 분석을 실습자료로 활용하고 있다.
1. 환자 사례
환자는 74세 남성으로 근육 관절을 많이 사용하는 육체노동을 하며, 흡연과 음주는 하지 않았다. 2010년 순환기내과에서 위부 팽만감, 숨차고 가슴에 심한 통증 증상으로 ‘I420 확장성 심근병증’진단을 받았고 처방약물 내역은 Table 1과 같았다. 이후 삼환계 항우울제 tianeptine 12.5 mg이 추가되었고, warfarin은 0.5~5 mg을 주기적으로 조정하여 처방 받았다. 또한 2012년 요추디스크 진단을 받은 이후부터 정형외과에서 소염진통제(aceclofenac 100 mg 또는 loxoprofen 또는 celecoxib 200 mg 또는 acetaminophen SR 650 mg), 근육이완제, 위점막 보호제를 간헐적으로 처방 받았으며, 때때로 만성통증 개선 목적으로 일반의약품 소염진통제도 구매하였다. 2017년 환자는 인후 이물감이 심하고 숨찬 증상이 심해져서 복용약물에 β-blocker와 statin이 추가되었으며, 2019년 출혈 직전까지 복용한 처방약물 내역은 Table 2와 같았다. 2019년 3월 환자는 항문출혈을 여러 번 호소하였고 ‘K649 치핵출혈’이라고 진단받았으며, 장기간에 걸쳐 복용중인 warfarin으로 인한 출혈 과다로 응급실 수혈 및 s-amlodipine 2.5 mg과 warfarin 3 mg 복용 중단 후 치료하여 출혈이 멈추었다.
2. 약사의 처방전 검토
환자는 ACEI, β-blocker, 이뇨제가 포함된 심부전 C단계에 해당하는 치료를 받고 있고, 복용중인 처방전 내 검토에서 처방약물의 용량은 적절하였으며, 약물-약물 상호작용 위험 가능성이 적음으로 확인하였다. Warfarin-ezetimibe는 prothrombin time (PT) 또는 international normalized ratio (INR)를 증가시킬 수 있고(보통), warfarin-rosuvastatin은 INR과 출혈위험을 증가시킬 수 있으며(보통), furosemide-
ramipril은 체위성저혈압(postural hypotension)을 일으킬 수 있다(보통)(Fig. 1).
다만, 같은 시기 타 병원에서 celecoxib 200 mg와 acetaminophen SR 650 mg를 처방 받은 내역으로 처방전 간 검토하였을 때 약물-약물 상호작용 위험 가능성이 높음을 확인하였다. Loop 이뇨제와 NSAIDS 병용은 이뇨효과를 감소시키고 신독성을 일으킬 수 있고(심각), 항응고제와 NSAIDS 병용은 출혈위험을 증가시길 수 있으며(심각), acetaminophen과 warfarin 병용은 출혈위험을 증가시길 수 있다(보통)(Fig. 2).

|
Fig. 1 Drug-drug interaction results of patient’s prescribed medications1) |

|
Fig. 2 Drug-drug interaction results of patient’s concurrent medications1) |
|
Table 1 Patient’s prescribed drug list by circulatory internal medicine (2010.06.) |
|
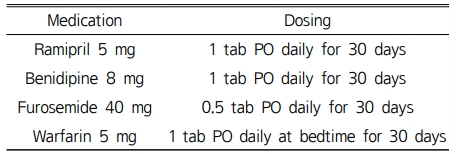
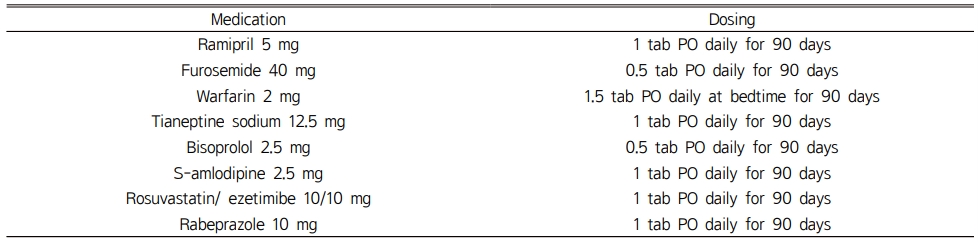
Table 2 Patient’s prescribed drug list by circulatory internal medicine (2018.12.) |
위 환자는 확장성 심근병증, 요추디스크, 치핵 출혈 등이 있는 74세 남성으로, 항응고제 warfarin과 NSAIDS 병용으로 인한 출혈위험이 있는 상태에서 치핵으로 인한 출혈이 위급하게 발생한 경우로, 대학병원 응급실에 방문하였으나 심장상태 불안정으로 수술이 불가하다고 하였고, 순환기내과 주치의가 있는 2차 의료기관에서 수술 치료하게 되었다.
대한부정맥학회와 AHA/ACC 가이드라인에 의하면 심방세동을 동반한 심부전 환자에서 추가적인 혈전 위험인자들이 있는 경우 항응고 약물을 투여하도록 추천하고 있으며, 심방세동 환자의 뇌졸중 위험도를 평가하는 CHA2DS2-VASc Score [Congestive heart failure, Hypertension, Age (65~74 yrs = 1 point, ≥75 yrs = 2 points), Diabetes, previous Stroke/transient ischemic attack (2 points), Vascular disease, Sex category (female)]를 기준으로 하고 있다. 환자는 CHA2DS2-VASc Score≥2인 경우에 해당하므로, 뇌졸중 및 혈전 색전증 예방을 위해서 warfarin을 투여한 것으로 추정할 수 있다.2,3) 하지만 유럽 심장학회의 HAS-BLED (Hypertension, Abnormal renal and liver function, Stroke, Bleeding history, Labile INR, Elderly>65, Drugs or alcohol) 출혈 위험 예측인자 중 나이(고령), 고혈압, 불안정한 INR, 출혈, 약물(NSAIDS) 등에 해당되어 HAS-BLED score ≥3이므로 출혈 위험성이 높은 고위험군으로, 항응고제로 인한 출혈 예방과 위험성 검토가 필요하다.4) 또한 환자는 warfarin을 복용하는 상태에서 NSAID를 주기적으로 복용했을 가능성을 추정할 수 있으며, NSAID 유발 출혈위험 인자 ≥ 2 (고령, 고용량 NSAIDS, 항응고제 병용)이므로 고위험군에 해당한다.5) 따라서 약물-약물 상호작용을 최소화하고 안전한 약물 사용을 위해 다음과 같은 중재가 권장된다.
1. 복용중인 warfarin 변경: novel oral anticoagulant (NOAC) 권고를 통한 출혈위험 감소
Warfarin은 vitamin K reductase를 억제함으로써 vitamin K-dependent carboxylase의 작용을 억제하고 이에 따라 다양한 단계에서 응고인자를 억제함으로써 혈액응고를 억제한다. Warfarin의 즉각적인 효과는 factor Ⅶ과 protein C를 고갈시키는 데에서 비롯되며, 이들의 반감기는 약 6시간이다. 그러나 factor Ⅸ, Ⅹa, Ⅱ의 반감기가 각각 24, 40, 60시간으로 길기 때문에 완전한 응고효과가 나타나는 데에 오랜 시간이 걸린다. 따라서 warfarin 사용중단 5-7일에 앞서 heparin을 이용한 단계적 처치가 요구된다. 또한 warfarin은 치료범위가 좁고 전반적인 출혈 위험 및 두 개내 출혈위험이 NOAC에 비해 높다는 단점이 있다. 다만 dabigatran은 warfarin에 비해 위장관 출혈위험이 높다.6,7) Warfarin은 CYP 2C9, 1A2, 3A4 등에 의해 대사되는 약물로 다양한 약물 및 음식과의 상호작용이 있고, VKORC1 유전자 다형성에 의해 warfarin의 개인별 용량 차이가 있으며, 치료효과가 나타나는 영역이 좁아 약물의 효과와 부작용 예측을 위해서 INR monitoring을 지속적으로 수행해야 한다. 반면 NOAC은 응고의 최종단계에서 prothrombin (factor Ⅹa)을 억제하거나 thrombin (factor Ⅱ)를 직접 억제하는 약물이다. 이러한 기전에 의해 용량에 대한 반응이 일정하게 나타나고 치료범위가 넓으며 약물 효과를 예측할 수 있다는 장점이 있다. Apixaban과 rivaroxaban은 factor Xa의 가역적, 선택적 억제제이며 dabigatran은 factor Ⅱa에 가역적인 억제제로 작용한다. NOAC은 warfarin에 비해 혈전생성억제 효율은 떨어지지 않으면서 출혈 부작용은 감소시키는 결과를 보인다. 또한 출혈 발생 시 중단할 때 빠른 지혈효과를 나타내고 warfarin에 비해 약물상호작용이 적고 정기적인 INR 모니터링이 필요하지 않다. NOAC은 항응고 효과를 모니터링하는 지표가 확립되어 있지 않다는 점이 단점으로 작용할 수 있으며, 기존의 activated partial thromboplastin time (aPTT), PT, INR 등의 지표는 NOAC에 사용될 수 없다.8)
2. NSAID 사용법 변경: 위장관 출혈위험이 낮은 NSAID 및 위장관 보호제 사용 권고
위장관 출혈위험과 심혈관 질환 위험이 높은 환자에서 NSAID 선택기준은 1) 비선택적 NSAID + 위장관보호, 2) 저용량 celecoxib + 위산분비억제제, 3) 마약성 진통제의 호흡부전과 의존성, NSAID에 의한 출혈, 심혈관질환 위험과 신장독성이 없는 tramadol, 4) 상대적으로 출혈위험이 적은 acetaminophen을 권고한다. 또한 일반의약품 진통제 구매 시 복용중인 통증약이 있는지 확인한다.9,10)
3. 지속적인 환자 교육 제공
Warfarin의 출혈 위험에 대한 교육, 출혈을 예방하기 위한 생활습관과 약물 교육을 제공한다. 혈뇨, 혈변, 상처에서 피가 그치지 않을 때, 이유 없이 쉽게 멍이 들거나 피부에 자반이 나타나는 등은 이 약의 효과 과다로 인해 나타나는 출혈 증상이므로, 이상반응이 나타날 시 의사나 약사에게 알린다. 주의사항으로 치과치료 또는 내시경검사 등 출혈이 예상되는 시술을 받을 시 이 약의 복용을 의사에게 반드시 알리고, 상처를 입힐 수 있는 운동이나 행동을 삼가도록 한다. 특히 warfarin 복용환자의 식이습관에 대해서 녹즙 또는 청국장 등 비타민 K가 들어있는 식품은 한꺼번에 다량 섭취하지 않고, 가급적 일정한 양을 섭취하도록 안내해야 한다. 또한 다른 약국에서 일반의약품(진통제) 구매 시 warfarin 복용 중임을 언급하도록 안내한다.
본 환자의 경우 warfarin 관련 출혈 이후, warfarin 3 mg을 40일간 복용 중지하였고 2019년 4월 edoxaban 30 mg (상품명 릭시아나)으로 처방 변경되었다. 2020년 5월 ‘I420 확장성 심근병증’, ‘I481 지속성 심방세동’으로 진단받아 edoxaban 30 mg, amlodipine 5 mg/olmesartan 20 mg/rosuvastatin 10 mg 복합제, bisoprolol 1.25 mg, tianeptine 12.5 mg, pantoprazole 20 mg으로 약물처방을 유지하고 있다.
본 증례보고는 심근병증 환자의 10년간 약물복용 내역을 추적 조사하여 warfarin의 출혈 위험성과 약물상호작용 확인을 통해서 지역약국에서 환자복약관리가 매우 중요함을 체험할 수 있는 의미 있는 사례였으며, 약학대학생의 약국 실무실습 교육 중 발생하여 학생이 직접 사례에 대해 조사를 하며 관련 문헌을 찾아보고 약사의 적절한 중재 방안에 대해 프리셉터와 논의를 하는 방식으로 학생 실무실습 교육에 활용되었다는 점에서 의미가 있었다. 약국실무실습 프리셉터로서 실습기간 중에 환자사례를 발견하고 열심히 연구한 학생에게 고마움을 표하는 바이며, 그 과정에서 방향을 찾아갈 수 있도록 안내하는 역할을 할 수 있어서 기쁘게 생각한다.
- 1. https://www.micromedexsolutions.com/micromedex2/librarian/deeplinkaccess?source=deepLink&institution=SZMC^SZMC^T43537. Accessed in May 28, 2019.
- 2. 2018 대한부정맥학회 심방세동 치료 가이드라인, http://www.k-hrs.org/P_Board_List_TypeQA_EDUCareinstructions.asp?LoadPage=P_EDUCareinstructions. Accessed in May 28, 2019.
- 3. https://www.acc.org/guidelines. Accessed in May 28, 2019.
- 4. 민보경, Arrhythmias. In; Pharmacotherapy Part 1, 3rd Ed, Shinilbooks, 2014:261-5.
- 5. Lanza FL, Chan FK, Quigley EM; Practice Parameters Committee of the American College of Gastroenterology. Guidelines for prevention of NSAID-related ulcer complication. Am J Gastroenterol 2009;104(3):728-38.
-

- 6. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139-51.
-
- 7. Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L; Randomized Evaluation of Long-Term Anticoagulation Therapy Investigators. Newly Identified Events in the RE-LY Trial: N Engl J Med 2010;363:1875-6.
-
- 8. Pollack CV Jr, Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal, N Engl Med 2015;373:511-20.
-
- 9. Seoul National University, College of Pharmacy Fourth year. Musculoskeletal disorders, Clinical Pharmacy 2019-2020.
- 10. Chisholm-Burns MA. Pharmacotherapy Principles & Practice. 4th edition. 2016. McGraw-Hill Education.
 This Article
This Article
-
2021;7(1):30-33
Published on May 31, 2021
- Received on May 17, 2021
- Revised on May 29, 2021
- Accepted on May 31, 2021
Services
Shared
Correspondence to
- Jun Woo Lee
-
Gangseo-gu gomdallae-ro 226, Gomdallae Pharmacy, Seoul, Republic of Korea
Tel: +82-2-2642-4196, Fax: +82-2-2655-0381 - E-mail: sygom@hanmail.net
04310 서울특별시 용산구 청파로47길 100 (청파로 2가) 숙명여자대학교 약학대학 308호
308 College of Pharmacy, 100, Cheongpa-ro 47-gil, Yongsan-gu, Seoul, 04310, Republic of Korea
FAX : 02-710-9799 Email : koacp@koacp.org